Ground Realities of Digital Healthcare in Switzerland: How General Practitioners Work with the Electronic Patient Record
A practice-based look at why Swiss GPs use the Electronic Patient Record selectively and what makes digital health infrastructure workable in everyday care.

Topic
This master's thesis examines how Swiss general practitioners work with the Electronic Patient Record (EPR) in everyday clinical practice. Rather than simply determining whether the EPR is adopted or rejected, the study investigates how general practitioners (GPs) incorporate it into specific work situations, how they respond to practical challenges, and why EPR use stabilizes in some contexts but remains selective or absent in others. The thesis focuses on the practical realities of digital health infrastructure in Swiss primary care.
Relevance
The Swiss EPR is intended to improve information exchange, coordination, and continuity of care. However, its value in primary care depends on its workability in everyday practice. For GPs, digital information must be accessible, reliable, clinically relevant, and compatible with time-constrained workflows. Therefore, understanding how practitioners use, bypass, or adapt the EPR is important because digital infrastructures create value only when they become workable in everyday clinical practice.
Results
The findings show that, while the EPR is formally available, it has not yet been practically incorporated into everyday primary care. GPs do not routinely adopt or simply reject it. Instead, they use it selectively, especially when broader patient information is needed for complex, chronic, or information-intensive cases. This selective use is shaped by fragmented information flows, limited provider and patient participation, weak integration with practice software, manual work, and reliance on parallel infrastructures. EPR information only becomes clinically useful when GPs can interpret, filter, and responsibly integrate it into care.
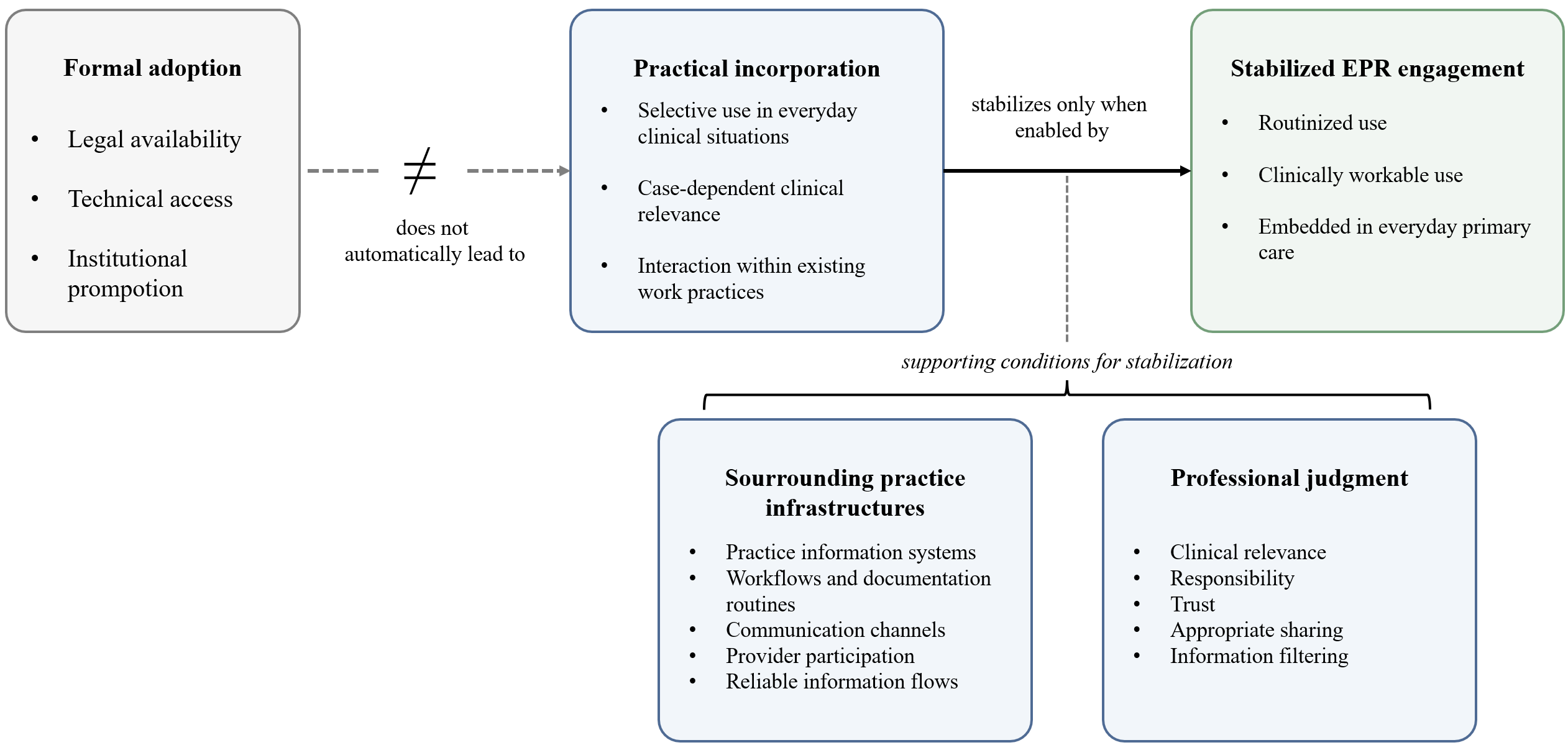
This figure illustrates the central finding of the thesis: formal availability does not automatically lead to stable EPR engagement. Practical incorporation occurs only when the EPR is supported by existing work routines, surrounding practice infrastructures, and professional judgment.
Implications for practitioners
- Integrate the EPR more deeply into existing practice information systems to reduce the need for separate logins, manual uploads and downloads, and duplicate documentation.
- Prioritize structured data, clinical summaries, metadata, search functions, and meaningful filtering over large collections of PDF documents.
- Strengthen participation across providers, laboratories, pharmacies, and patients so that the EPR becomes a reliable source of relevant information.
- Support patient onboarding, access rights, permissions, and delegated tasks so that administrative work is not shifted unnoticed into primary care.
- Treat EPR implementation as an ecosystem-level challenge, not just a technical rollout or user adoption problem.
Methods
The study employed a qualitative, interpretive research design. The empirical material consisted of six semi-structured interviews with Swiss general practitioners and five publicly available practitioner accounts from podcasts, media interviews, and professional articles. The analysis focused on concrete situations, frictions, work adaptations, and patterns of EPR engagement in everyday clinical practice. The data were analyzed using the Gioia methodology to develop first-order concepts, second-order themes, and aggregate dimensions. The study was theoretically informed by Orlikowski’s practice lens and the concept of deep structure use.